![]()
![]()
Fast, modern disease mapping. SDALGCP2 fits a
spatially discrete approximation to a log-Gaussian Cox process
(SDA-LGCP) to spatially aggregated disease counts, with
a one-line, glm-like interface and C++ speed. The method is
described in Johnson, Diggle & Giorgi (2019, Statistics in
Medicine, doi:10.1002/sim.8339).
# install.packages("remotes")
remotes::install_github("olatunjijohnson/SDALGCP2")You need a C++ toolchain (Rtools on Windows, Xcode CLT on macOS) because the performance-critical kernels are compiled.
data is an sf object whose columns hold the
response, covariates and offset. Everything else (candidate-point
spacing, the spatial scale, MCMC settings) is chosen automatically.
library(SDALGCP2)
fit <- sdalgcp(cases ~ deprivation + offset(log(population)), data = regions)
summary(fit) # glm-style coefficient table + spatial parameters
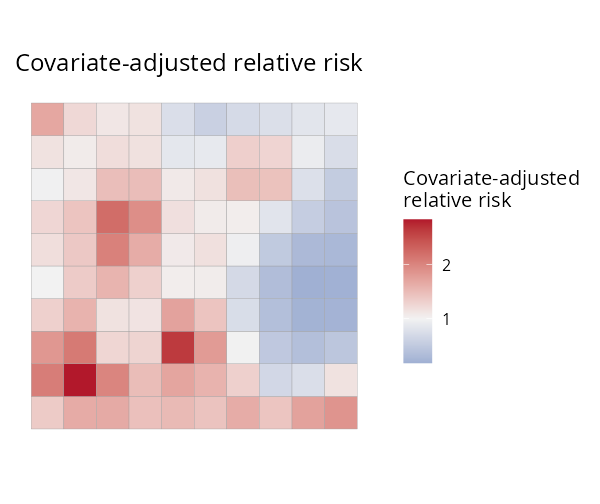
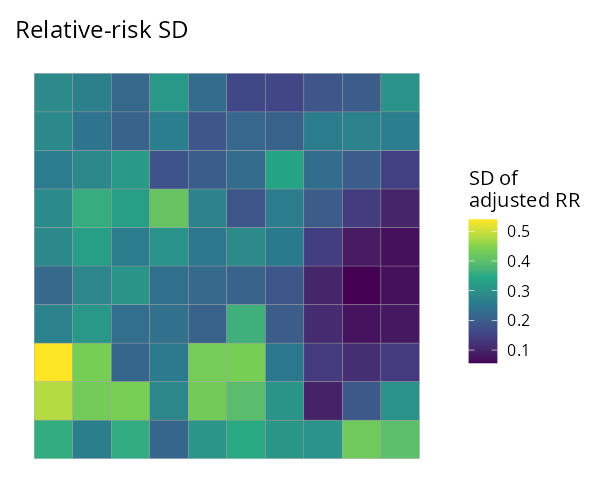
rr <- predict(fit) # an sf: relative_risk, relative_risk_se, adjusted_rr, adjusted_rr_se
plot(fit) # relative-risk map
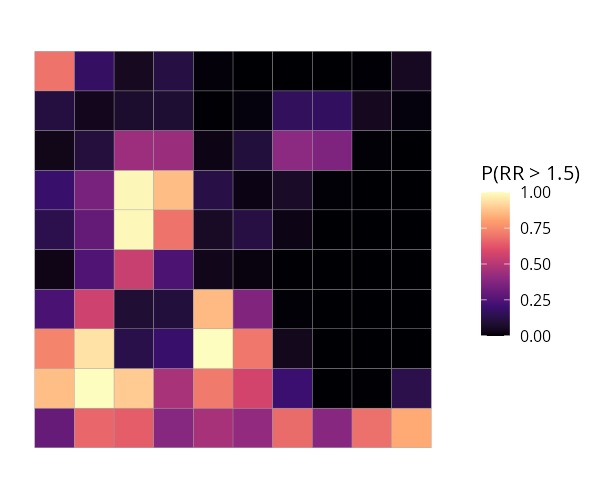
plot(fit, "exceedance", threshold = 1.5) # hotspot probabilitiesThat is the whole workflow. The same sdalgcp() call also
covers:
| You want… | Add… |
|---|---|
| raster (continuous) covariates | rasters = my_raster (enter on the intensity scale) |
| a spatio-temporal model | time = "year" |
| population-weighted aggregation | popden = pop_raster |
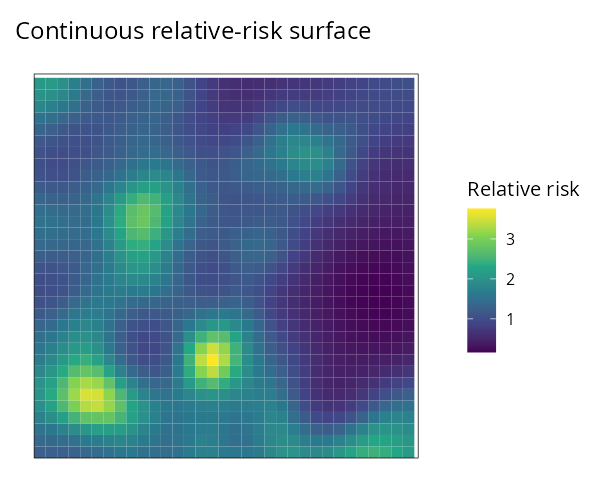
| Relative risk | Uncertainty (SD) | Exceedance P(RR > 1.5) | Continuous surface |
|---|---|---|---|
|
 |
 |
 |
sdalgcp(formula, data) — feels
like glm(); sensible defaults so a first fit needs no
tuning.φ
is optimised continuously by default (no grid), with a proper standard
error — see the derivation
PDF.(N·T)² covariance.See the package website for worked, reproducible articles:
scale = "grid") vs continuous
(scale = "continuous") φ.Johnson, O., Diggle, P. & Giorgi, E. (2019). A spatially discrete approximation to log-Gaussian Cox processes for modelling aggregated disease count data. Statistics in Medicine 38, 4871–4887.